by Bob Buddemeier
 Did you ever stop to wonder about the on-line journal that you’re reading? If not, it may be time to switch to a different article, but if so, read on.
Did you ever stop to wonder about the on-line journal that you’re reading? If not, it may be time to switch to a different article, but if so, read on.
The Complement was built by David Gordon of Ashland Websites, who continues to coach us and troubleshoot as needed. No, he doesn’t work for free, but it turns out that this is a remarkably cheap hobby compared to many.
Under the hood, it is powered by WordPress software running on the Bluehost site. That’s a giant ho-hum for most people, but it’s worth mentioning because those pieces of software account for a remarkably large percentage of the cottage-industry blogs and websites around the world.
The dedicated editorial team consists of Joni Johnson, Connie Kent, Tom Conger, Reina Lopez (photographer), and yours truly. That is far from all, however. We offer frequent contributions from Nit-Wit Newz correspondent A. Looney, Russy Sumariwalla, and our outstanding panel of book reviewers (Anne Newins, Bonnie Tollefson, Jan Hines, Liz Caldwell, Connie Kent, Sally Densmore, and Leslie Schettler). We’ve also had contributions — both written and pictorial — by and about many RVM residents.
What can we do? Well, we can post pictures, videos, downloadable PDFs (and other formats), and plain old click-and-read articles. The zippy thing is that we can do it fast and easily — from a final draft in Word to an on-line article can be a matter of minutes — which means we get to concentrate on the fun and exciting parts of journalism instead of bogging down in process and procedure. As far as we can tell, our readers appreciate that as much as we do.
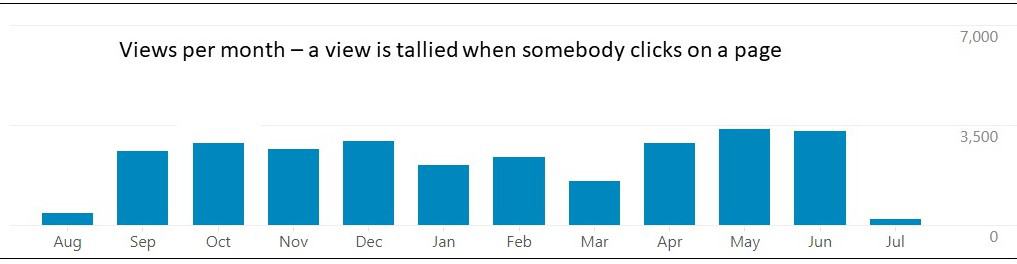
And how much do those readers read? The figure below shows monthly views — the total number of articles (posts) that get clicked (whether or not they actually get read). Over 3,000 — not bad, we think. How many actual human beings does that represent? A visit is one person coming to the site (no matter how many posts s/he views). We get 300-ish in the first few days after an issue comes out, and if we announce a mid-month feature or even just put out a reminder, we get another pulse about half as big. The trouble is, we have no way of knowing how many visits are due to a few insatiable people coming back again and again. We think around 300 is a conservative estimate of individual viewers.
What can’t we do? We can’t provide for the non-computer (or non-internet) users. We’ve looked at it, and it is just too costly — in time and effort as much as in dollars. Actually, let’s be honest. We won’t do that, because we aren’t interested in replacing our writing and thinking and editing time with formatting and copying and distribution. Sorry.
Another thing we can’t do is get to the computer-users who do not look at RVMlist — at least not without going to hit-everybody email blasts, which is really pretty obnoxious. We do offer a “subscription list” to anyone who wants to get a personal email when the RVMlist notice goes out — just give one of us your email, or send a request to openinforvm@gmail.com.
And finally, we can’t (or again, won’t) connect to myRVM, because the conditions for doing that aren’t consistent with our view of how an independent publication should operate.
Let’s take a look at expectations and actuality. We set up the structure with three main subdivisions — Arts & Info, News & Views, and Prepare.
Arts & Info was envisioned as the place for resident products — we started out with some poems by RVM poets past and present, and haven’t done that again largely because we’ve had enough other items (we figure 3-4 major ones plus some shorter notes or links for N&V and A&I — fewer for Prepare). We try to have at least one visual feature, and something on the lighter side each month, at least one book review and the library display, the program schedule, and whatever else comes along. We could run more some months, but we have actually had people tell us that we put out so much they have trouble getting around to reading it all.
New and Views = facts and opinions; in fact, quite a few of our resident-authored products end up here rather than in A&I because of their focus on a current issue (for example, Asifa Kanji’s “I am Not a Racist, They are“). We also have how-tos (grocery delivery), general community descriptions (solstice religious holidays), and resident concerns (what happens on hospital discharge). There are a few glimpses of the outside world — links to the Seattle and Portland Mirabella newsletters, which are very different products providing a look at other PRS facilities. We also offer links to and reprints of other items of interest; in this issue we reprint an article from the Seattle Mirabella Monthly on one of their residents who contributed to the translation of the Bible into Hawai’ian Pidgin.
Prepare was — and is — envisioned as a repository of accessible and RVM-relevant information on preparedness for emergencies and disasters. A lot of material has been accumulated there, but we have been marking time during the pandemic because we can’t refine resident plans or instructions until we have a clear picture of RVM emergency plans. Fortunately, the RVM planning process is within a very few months of being complete, and we expect to be making major updates to the information on the Prepare page. In the meantime, we have been focusing on Wildfire Season issues, which deserve everyone’s attention.
It seems to be going pretty well, but we would like to get more public feedback — there have only been 44 comments posted. Some have been substantive, like Doyne Mraaz’s comment on Russy Sumariwalla’s reprinted article, but the overall public number is few. We get far more personally — for example, only two of the 15 remarks in Life’s End Comments were posted publicly; the rest are anonymized personal communications.
Now — the latest — what about VIEWPOINTS? We wish we could tell you. We launched it with the conviction that there was another level of candor and debate needed beyond what we were providing with The Complement. We also launched it with a lot of internal debate and soul-searching and concern about how to to link it to or detach it from The Complement so as to maintain separate personalities. Well, silly us. We published a suite of articles on perceived failings in PRS/RVM management vis-a-vis the residents, and another article on one of the most problematic loci of ethnic and geopolitical strife, and guess what? The crowds with torches and pitchforks completely failed to materialize. We suspect that this does not mean that RVM is one giant nest of harmony and agreement, but rather that the residents have rather quickly self-selected into readers or non-readers.
providing with The Complement. We also launched it with a lot of internal debate and soul-searching and concern about how to to link it to or detach it from The Complement so as to maintain separate personalities. Well, silly us. We published a suite of articles on perceived failings in PRS/RVM management vis-a-vis the residents, and another article on one of the most problematic loci of ethnic and geopolitical strife, and guess what? The crowds with torches and pitchforks completely failed to materialize. We suspect that this does not mean that RVM is one giant nest of harmony and agreement, but rather that the residents have rather quickly self-selected into readers or non-readers.
It’s nice to be appreciated, but talking only to those who agree with you does not provide much of a feeling of advancing the total of human understanding. Since we didn’t make a specific schedule commitment for VIEWPOINTS, we’ll let it go fallow for a little while and see if something or somebody turns up. It could be you — think about it.






 delivery of tables and chairs on the day of their gathering. They publicized their “Neighbors Together” with a flyer given to each resident and signage placed at the end of their street on the day of the event. The signage was designed and supplied by the Marketing Department.
delivery of tables and chairs on the day of their gathering. They publicized their “Neighbors Together” with a flyer given to each resident and signage placed at the end of their street on the day of the event. The signage was designed and supplied by the Marketing Department.  The signs have been designed to be able to pass from one neighborhood to another. Drinks were BYOB and foods were kept to a minimum. Bag snacks were purchased at Costco
The signs have been designed to be able to pass from one neighborhood to another. Drinks were BYOB and foods were kept to a minimum. Bag snacks were purchased at Costco  and put in inexpensive plastic bowels found at the dollar store. With ease and simplicity, the party was born!!!! I arrived a few minutes after four and the gaiety was in full swing. For all that showed up, the joy was apparent. People were just plain happy to be together. Even with a less than stellar air quality, the slight breeze at 4 pm made it all quite comfortable. Some people kept their masks on as a caution against either the smoke or the Delta variant.
and put in inexpensive plastic bowels found at the dollar store. With ease and simplicity, the party was born!!!! I arrived a few minutes after four and the gaiety was in full swing. For all that showed up, the joy was apparent. People were just plain happy to be together. Even with a less than stellar air quality, the slight breeze at 4 pm made it all quite comfortable. Some people kept their masks on as a caution against either the smoke or the Delta variant. Orleans warned that residents would have to look after themselves for a while.
Orleans warned that residents would have to look after themselves for a while. It does not mean that we can function as policemen, firefighters, or paramedics. Set aside the technical aspects of emergency response — what it does mean is that your neighborhood or floor coordinator will be at your door sooner than RVM staff, and that in many cases your next-door neighbor can be there sooner still. Does somebody need an explanation of what’s going on, or what to do? Help with crating a pet? Assistance getting a walker and go-bag out to the driveway for pickup?
It does not mean that we can function as policemen, firefighters, or paramedics. Set aside the technical aspects of emergency response — what it does mean is that your neighborhood or floor coordinator will be at your door sooner than RVM staff, and that in many cases your next-door neighbor can be there sooner still. Does somebody need an explanation of what’s going on, or what to do? Help with crating a pet? Assistance getting a walker and go-bag out to the driveway for pickup? yourselves.” Initially RPG focused heavily on preparations for the Cascadia earthquake. The 2020 wildfire evacuation experience refocused attention on emergency response, but now that the shelter-in-place policy has been put forward, it’s time to revisit preparation. There are more different kinds to consider — short-distance and short-time shelter, as well as the long haul following an earthquake.
yourselves.” Initially RPG focused heavily on preparations for the Cascadia earthquake. The 2020 wildfire evacuation experience refocused attention on emergency response, but now that the shelter-in-place policy has been put forward, it’s time to revisit preparation. There are more different kinds to consider — short-distance and short-time shelter, as well as the long haul following an earthquake.



 account “my_aussie_gal” in August when Secret was just shy of her 8 month birthday. She chose an Australian shepherd because they are known to have a strong work drive and according to the American Kennel Club, they are remarkably intelligent, quite capable of hoodwinking an unsuspecting novice owner and a brainy and a tireless trainable partner for work or sport.
account “my_aussie_gal” in August when Secret was just shy of her 8 month birthday. She chose an Australian shepherd because they are known to have a strong work drive and according to the American Kennel Club, they are remarkably intelligent, quite capable of hoodwinking an unsuspecting novice owner and a brainy and a tireless trainable partner for work or sport. fall majoring in Japanese with her service dog, Secret, beside her. She says in her interview with Newsweek that she couldn’t have made it through her community college classes without Secret. Mary started her journey as a home-schooled child. When she started her Instagram account, she hoped her followers might help her with some teaching tips. She spent a year training Secret as a therapy dog. Then the training took off.
fall majoring in Japanese with her service dog, Secret, beside her. She says in her interview with Newsweek that she couldn’t have made it through her community college classes without Secret. Mary started her journey as a home-schooled child. When she started her Instagram account, she hoped her followers might help her with some teaching tips. She spent a year training Secret as a therapy dog. Then the training took off.